Client Alerts & Insights
CMS Bets on the Long Game with 10‑Year LEAD ACO Model
April 14, 2026
Practices:
Key Takeaways for Accountable Care Organizations (ACOs):
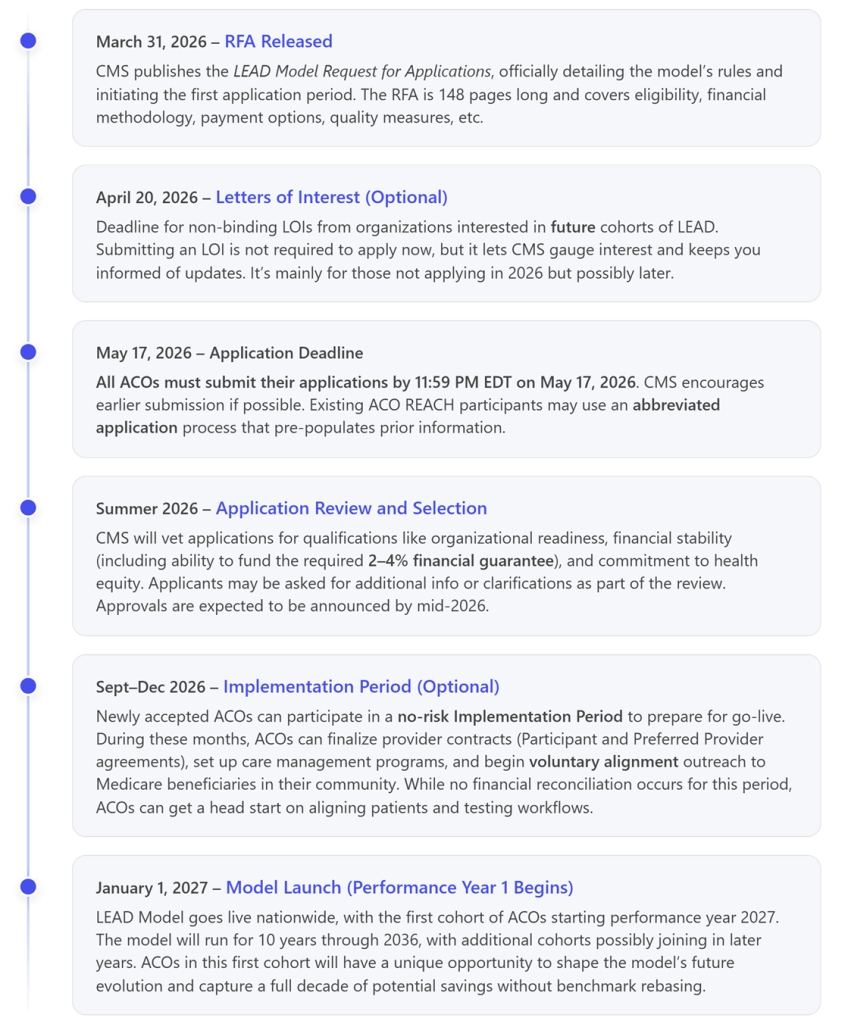
- New 10-Year ACO Demo (2027–2036): Starting January 1, 2027, providers will have the opportunity to participate in a decade-long, voluntary ACO program with no benchmark rebasing throughout the 10-year span [1]. The Long-term Enhanced ACO Design (LEAD) Model will replace ACO REACH when it ends on December 31, 2026. CMS released the Request for Applications (RFA) on March 31, 2026, and ACOs must apply by May 17, 2026, to join the first performance year starting January 1, 2027.
- Stable Benchmarks & Two Risk Tracks: LEAD provides participating ACOs with a fixed historical spending baseline for the entire model duration (annual trend updates, but no mid-model resets). ACOs can choose between risk two tracks – a Global Risk Option (Global) (100% shared savings/losses) or Professional Risk Option (50% shared savings/losses), similar to ACO REACH. Global ACOs face a small benchmark discount (~1.75–3%) but get maximum reward potential [2], while Professional ACOs have lower risk and no discount on benchmarks.
- Broader Provider Participation – New Flexibilities: LEAD is designed to attract a wider range of providers – including small, independent and rural practices, specialty groups and new entrant ACOs – by lowering barriers that previously deterred participation. The model offers enhanced upfront cash flow and payment options:
- ACOs may receive capitated payments (for primary care or even all services)
- Advanced monthly payments are available to invest in care coordination
- A unique Non-Primary Care Capitation (NPCC) mechanism enables true specialist sub-capitation, giving specialist providers a fixed monthly payment and financial accountability for their services
- A 1.5% “administrative add-on” payment is afforded to ACOs with higher baseline spending (often those in high-need or rural areas), which does not have to be repaid.
- Specialist Integration via CARA: To further engage specialist physicians in ACOs, LEAD introduces CMS-Administered Risk Arrangements (CARA) [3]. Through CARA, an ACO in the Global track can contract with specialists on specific episode-based risk arrangements – for example, bundled cost targets for cardiac surgeries or oncology care – with CMS handling reconciliation of those arrangements. This allows specialists to share in savings or losses for episodes of care while easing the administrative burden (CMS provides the data and payment infrastructure). CARA will phase in starting 2028 and includes episodes for chronic conditions (e.g. CKD, ESRD) and even a “falls prevention” home care episode to help frail seniors safely age in place.
- Focus on High-Needs Populations & Equity: All LEAD ACOs will manage high-needs patients (e.g. those with multiple chronic conditions, frailty, or dual Medicare/Medicaid eligibility) as part of their aligned population, rather than in a separate track. The model uses concurrent risk adjustment and a separate spending trend for these complex patients to set realistic benchmarks [4]. If an ACO’s population is over 40% high-needs beneficiaries, CMS will lower the minimum number of patients required to participate, recognizing the smaller panels typical for providers focusing on complex patients. LEAD also continues beneficiary engagement incentives from prior models. For example, ACOs can offer Part B cost-sharing support (waiving copays for certain services) and, by 2029, may even subsidize part of patients’ Part D drug premiums to encourage preventive care and medication adherence.
- Application & Participation Requirements: Interested ACOs must apply by May 17, 2026. Like historical models, to be eligible, an ACO must be a legal entity capable of bearing risk and generally needs 5,000+ aligned Medicare lives (though high-needs-focused ACOs can qualify with fewer). Participants must use Certified EHR technology and have robust compliance and care coordination programs. A financial guarantee (reserve) is required to cover potential losses, typically 2-4% of the ACO’s Medicare Part A and Part B revenue (exact amount varies with the chosen risk track and capitation options). Notably, current ACO REACH participants can use a streamlined “abbreviated” application to transition into LEAD. CMS is also accepting non-binding Letters of Interest (LOIs) by April 20, 2026, from organizations that might join later cohorts.
- Timeline & Launch: CMS will notify accepted applicants by mid-2026. Those ACOs can participate in an Implementation Period (Sept–Dec 2026) with no financial risk, to establish provider networks and conduct beneficiary outreach before the model go-live. Performance Year 1 begins January 1, 2027, running in parallel with other CMS programs like MSSP. LEAD is expected to be the main option for risk-bearing ACOs in FFS Medicare through 2036, making 2027 a pivotal year for ACO strategy.
A New 10-Year Model to Succeed ACO REACH
The Long-term Enhanced ACO Design (LEAD) Model is the Center for Medicare and Medicaid Innovation’s (Innovation Center) next-generation accountable care initiative, created to succeed the ACO REACH model in 2027. Announced in late 2025 and detailed in an RFA on March 31, 2026, LEAD will launch on January 1, 2027 – exactly as ACO REACH sunsets – and run through 2036. This 10-year duration makes LEAD the longest-running ACO test ever undertaken by CMS. Importantly, CMS has committed that an ACO’s financial benchmark in LEAD will not be “rebased” or reset for the entire 10-year period. Instead, each ACO gets a fixed historical spending baseline (likely based on 2024–2026 costs for the first cohort) that will be updated annually by a blend of national/regional growth factors – but without the typical mid-model reset that, in past models, often shrank an ACO’s savings opportunity over time. This stable benchmarking is meant to encourage long-term investments in care improvement, since successful ACOs can retain the benefits of cost reductions for the full decade.
LEAD’s core mission is to expand the reach of accountable care to more providers and patients while sustaining the momentum of existing ACOs. CMS openly acknowledges that many providers (especially small, independent, rural, and physician-led practices) have been reluctant to join ACOs or have dropped out due to financial risk and administrative hurdles. LEAD directly addresses these issues. As CMS describes, the model is designed to reduce obstacles and “level the playing field” so that organizations of varying sizes and specialties can succeed in value-based care.
Key policy changes in LEAD include improved financial methodologies and new payment flexibilities to make ACO participation more attractive. For example, the RFA highlights that benchmarks will be more predictable and generous to high performers (no rebasing, plus adjustments for regional efficiency and prior savings). At the same time, upfront capitated payments are available to alleviate cash-flow concerns and fund care innovations. In short, CMS is signaling that LEAD is a more provider-friendly model intended to drive higher participation, including from groups that historically sat on the sidelines of ACO programs.
Risk Tracks: Global vs. Professional (100% vs. 50% Risk)
LEAD closely mirrors the two-tier risk structure of ACO REACH, offering ACOs a choice between:
- Global Risk: 100% shared savings and losses – the ACO is fully accountable for any cost overruns but keeps all savings beyond a threshold. In LEAD, Global ACOs will have a benchmark “discount” of about 1.75%–3% (i.e. CMS withholds a small percentage of the target up front as its share of savings). This discount is slightly lower than ACO REACH’s 3% flat discount and may be tapered for certain high-cost ACOs (the RFA suggests starting at ~1.75% for such ACOs and phasing up to 3%). In return, Global ACOs get maximum flexibility – they can opt for capitation of all Medicare payments (Total Care Capitation) and participate in the new CARA specialist risk arrangements (see below). A regional efficiency bonus (for historically low-cost ACOs) and a prior savings adjustment (crediting past ACO success) are also available only in the Global track, potentially boosting benchmarks for very efficient systems.
- Professional Risk: 50% shared savings and losses – a lower-risk option similar to a two-sided MSSP Track 1+. There is no discount applied to Professional ACO benchmarks, so these ACOs share savings from the first dollar. Professional ACOs can still choose Primary Care Capitation and advanced payment options for stable revenue, but they cannot access some Global-only features (like Total Care Capitation or CARA episodes). Notably, LEAD will require ACOs that start in the Professional track to remain at 50% risk for at least four years before they have an opportunity to switch to Global risk. This commitment ensures that lower-risk ACOs take time to build capabilities before potentially taking on full risk.
Both tracks will be evaluated on a common set of quality measures (a streamlined set of 7 measures, including claims-based metrics, CAHPS patient experience, and two electronic clinical quality measures to be phased in) with a 3% quality withhold applied to the benchmark that ACOs can earn back based on performance. This is a slightly smaller withhold than the 5% used in the final year of ACO REACH, reflecting an effort to make quality incentives meaningful but not overly punitive. High-performing ACOs will also be eligible for a “High Performer Pool” bonus, similar to REACH, and all participants must submit a Health Equity plan and a “Quality & Prevention” strategy outlining how they will improve preventative care and outcomes (especially for underserved groups).
New Payment Options for Predictable Cash Flow and Investment
To support a broader range of ACO participants, LEAD introduces and expands population-based payment mechanisms that provide predictable, up-front revenue in lieu of standard fee-for-service billing. All ACOs must select one of the following capitation payment mechanisms and should carefully consider which selection best fits its needs:
- Primary Care Capitation (PCC): All LEAD ACOs (Global or Professional) can opt for PCC, which pays the ACO a monthly per-beneficiary amount for primary care services delivered by its Participant Providers. This effectively pre-pays ~7% of the benchmark dedicated to primary care services. The capitation is adjusted for the ACO’s historical primary care spending and size, and it includes a built-in “Enhanced PCC” component (the greater of (i) the difference between 7% of the performance year benchmark and the estimated base PCC amount or (ii) 2% of the performance year benchmark) to inject additional resources for care management upfront. Providers continue to bill Medicare, but CMS reduces fee-for-service payments for primary care claims (by a percentage the ACO selects) since the ACO is getting paid separately. The PCC option is intended to strengthen primary care infrastructure – ACOs can use the steady cash to hire care coordinators, extend office hours, invest in data analytics, and otherwise improve patient outreach without worrying about visit-based revenue.
- Total Care Capitation (TCC): Available only for Global risk ACOs, TCC takes PCC a step further by providing a full per-member per-month payment for all Part A and B services for aligned patients, covering both primary and specialty care. In this model, 100% of an aligned patient’s Medicare claims from the ACO’s core providers are paid via the capitation (with an optional portion of claims from certain affiliated specialists or facilities also shifted into the capitation). TCC essentially turns the ACO into something akin to a fully capitated entity, with maximum flexibility in how it delivers care. Few ACOs are likely to adopt full TCC immediately, but it creates a path toward a Medicare Advantage-like structure within fee-for-service. ACOs in Global track that don’t elect TCC can still do PCC and have specialists on fee-for-service.
- Advanced Payment Option (APO): Similar to the “advanced shared savings” feature in ACO REACH, APO provides a monthly upfront payment to the ACO, which is later reconciled against fee-for-service claims. It’s essentially an advance on expected billings (sometimes called a “loan” against future payments). APO can help new ACOs with immediate cash for investments, but since it’s recouped from claims, it doesn’t change the total revenue, unlike true capitation.
- Non-Primary Care Capitation (NPCC): New in LEAD, NPCC is a form of sub-capitation for specialty care. If an ACO is in Primary Care Capitation, it can arrange for certain specialty providers (or even post-acute providers like skilled nursing facilities or home health agencies) to be paid a fixed monthly amount for treating the ACO’s patients, instead of billing per service. Importantly, these NPCC payments are not reconciled against actual fee-for-service use – they are prospective budgets for specialists. This gives specialists participating in an ACO a powerful incentive to manage cost-efficient care: if they keep costs under the capitation amount, they come out ahead, and if they overspend, they absorb losses. For example, an ACO could pay a cardiology group a flat per-patient fee to manage all cardiac care for its beneficiaries; the cardiologists then have flexibility to deploy care as they see fit (e.g., telemedicine check-ins, care coordinators) and benefit by avoiding unnecessary procedures or hospitalizations. NPCC is an optional tool, but it signals CMS’s intent to involve specialists as true partners in cost accountability – a notable evolution from prior models that focused mostly on primary care.
- 1.5% Administrative Payment (“Add-On”): To encourage participation by higher-cost providers and those caring for complex, underserved communities, LEAD offers a small additional payment to boost financing for care improvements. ACOs with baseline spending above their region’s average will receive a monthly payment equal to 1.5% of their benchmark. Unlike other upfront payments, this does not need to be repaid or reconciled later – it is essentially seed money to invest in things like staffing, data systems, or ACO infrastructure that help lower costs over time. This policy is aimed at ACOs with historically high-cost populations (for example, areas with severe social needs or limited access to care); these organizations often have the greatest opportunities for savings, and the 1.5% add-on gives them the capital to get started.
These payment options can be mixed and matched. For instance, an ACO in the Global track might choose TCC for core providers (full capitation) or stick to PCC and use NPCC capitation with certain specialists. All ACOs, regardless of track, can use APO, and eligible ACOs automatically get the 1.5% add-on if they qualify. The bottom line for ACOs is that LEAD offers far more flexibility in cash flow than any prior Medicare ACO model – addressing a top concern of smaller practices and hospitals that lack the reserves to wait a full year for shared savings.
Embedding Specialists and High-Needs Care into ACOs
A major theme in LEAD is integrating care for special populations – both in terms of providers (specialists) and patients (those with complex needs). The model breaks new ground in how it brings these traditionally challenging elements under the ACO umbrella:
- Specialist Engagement – CARA Episodes: Under the voluntary CMS-Administered Risk Arrangements (CARA) program, LEAD’s Global ACOs can formally partner with specialty providers in managing the costs of specific episodes of care. In practice, an ACO and a specialist (or specialist group) will agree on a target price for a defined clinical episode (e.g., an orthopedic surgery plus 90-day recovery). The specialist then shares in savings or losses relative to that episode cost target, with CMS calculating the performance and handling payments on the back-end. CARA thus gives specialists a direct financial stake in cost outcomes – motivating them to avoid complications and expensive, low-value services – while relieving ACOs from having to administer complex bundled payment contracts themselves. CMS will roll out standard definitions for many episodes by 2028 (including chronic condition episodes for diabetes, heart failure, chronic kidney disease (CKD), etc., and procedure bundles for surgeries). A particularly innovative example is a CARA-sponsored “Rise to Age in Place” episode to prevent falls in homebound frail elders (covering home safety assessments, modifications, and other services). For ACOs, CARA is an opportunity to deepen collaboration with specialists – aligning incentives in ways that ACOs alone often struggled to do – and to potentially improve quality and patient experience in high-cost specialties.
- High-Needs Beneficiaries: Unlike ACO REACH, which had a separate High Needs ACO model for organizations enrolling exclusively complex patients, LEAD incorporates care for high-needs Medicare beneficiaries into all ACOs. This means any LEAD ACO can have a mix of regular and high-needs patients (including those with serious chronic conditions, functional limitations, or dual Medicare-Medicaid status). The model adjusts for this by using a concurrent risk adjustment approach for high-needs patients (to more accurately reflect their current severity) and by applying a more generous spending growth trend factor for communities with many high-needs enrollees. Additionally, if an ACO’s aligned population is at least 40% high-needs, the minimum beneficiary count requirement is reduced (the RFA doesn’t specify exact numbers publicly, but such ACOs might only need roughly 1,000–2,000 patients instead of 5,000). This makes it feasible for specialty-led ACOs or regional programs focusing on frail elders, serious illness, or medically complex patients to participate in LEAD.
- Health Equity: All LEAD ACOs will be expected to implement strategies to address health equity and social needs. For example, participants must submit a Health Equity Plan (similar to REACH) outlining how they’ll identify and reduce disparities in their patient population. The model also broadens certain benefit enhancements that can directly help patients: e.g.,ACOs can pay for transportation for treatment or home health visits after hospitalizations, provide chronic disease self-management rewards (like nutrition and wellness programs), and starting in 2029, even offer Part D premium discounts for their patients. These tools, combined with the financial incentives to keep high-risk patients out of the hospital, align the ACO’s success with improved care for the most vulnerable groups – a clear priority for CMS.
Application Timeline and Key Requirements
The window is now open for the first round of LEAD applications. Below is an outline of the key dates and steps for ACOs considering this opportunity:
Eligibility & Compliance Essentials: To be accepted into LEAD, an ACO must meet rigorous standards similar to other Innovation Center models. Key requirements include:
- Minimum Population: Generally 5,000 Medicare fee-for-service beneficiaries must be aligned to the ACO at the start of each performance year. (ACOs with a high share of complex, high-needs patients can qualify with a smaller population, as noted above.) The ACO should have a strategy to maintain or grow alignment over time, including leveraging voluntary alignment of patients who designate the ACO’s providers as their primary clinicians.
- Organizational Structure: The ACO must be a legal entity capable of entering into a Participation Agreement with CMS and bearing risk. It must have a governing board with at least 75% control by participating providers (and at least one Medicare beneficiary representative). The ACO needs a robust compliance plan and cannot include any providers or owners who are excluded or “prohibited participants” (e.g., organizations with certain fraud convictions).
- Whole-TIN Participation: In a shift from ACO REACH’s flexibility, LEAD requires core participants to join at the Tax Identification Number (TIN) level – if a practice’s TIN is in the ACO, all providers billing under that TIN are considered ACO participants. This is similar to MSSP and prevents cherry-picking individual doctors. ACOs should plan accordingly, perhaps carving out separate TINs for providers they don’t want in the ACO. (Preferred Provider arrangements, however, can still be at the NPI level for more limited relationships.)
- Financial Guarantee: Before starting, an ACO must demonstrate the ability to repay losses by establishing a reserve or financial guarantee (in the form of escrow funds, a line of credit, or a surety bond). The required amount is tied to the ACO’s size and risk level – roughly 2% of prior-year Part A/B spending for a Professional ACO, and 4% for a Global ACO with full capitation (the exact formula is detailed in the RFA). This is higher than what was required under ACO REACH, reflecting the longer performance period and greater potential payouts in LEAD. ACOs should be prepared to secure this collateral by late 2026, if accepted. CMS also offers an Extended Repayment Option for any ACO that incurs losses but remains in the model, allowing them to pay back Medicare over time to avoid immediate financial strain.
- Data and Tech Capabilities: Participants must use Certified EHR Technology and be able to report electronic clinical quality measures by the later years of the model. ACOs will be expected to submit detailed data to CMS, including quality metrics and information on social determinants of health efforts. CMS is launching a “Tech Enabler” program within LEAD to assist ACOs (especially smaller ones) in adopting high-value digital health tools and data sharing capabilities. This is in line with CMS’s push to make sure even physician-led ACOs have the IT infrastructure to manage population health effectively.
- Overlap Restrictions: An organization cannot participate in both LEAD and another shared-savings model with the same providers. For example, physicians in a LEAD ACO generally cannot simultaneously be in the Shared Savings Program or in another Innovation Center model with total-cost-of-care accountability. However, beneficiaries aligned to a LEAD ACO can still be part of certain other initiatives (like stand-alone disease-specific models or primary care programs) as long as there’s no double-counting of savings – CMS will provide guidance on permitted overlaps.
For current ACO REACH participants: CMS has made it easier to carry on in LEAD by offering an abbreviated application that pre-fills much of the information from your REACH participation. If you’re in good standing and your organization’s structure remains largely the same, the review will focus on any new aspects of LEAD (such as confirming your choice of risk track and payment options, and ensuring you can meet the new financial guarantee requirements). It’s highly recommended that REACH ACOs take advantage of this opportunity to seamlessly transition and avoid any gap in participation. ACO REACH will not continue beyond 2026, so without a LEAD application, current REACH organizations would need to revert to MSSP or fee-for-service – a disruptive step backward for organizations used to the flexibility of the Innovation Center model.
Preparing for LEAD – Action Items for ACOs
LEAD represents a significant commitment – a decade-long endeavor with new rules – but also a chance at unprecedented stability and support in the Medicare ACO space. As one analysis observed, 2027 will be a pivotal year as ACO REACH winds down and LEAD begins, requiring organizations to decide how to position themselves in the evolving landscape of value-based payment. Every ACO (and would-be ACO) should consider the following actions in the coming weeks:
- Evaluate Strategic Fit: Review the LEAD RFA and assess how the model’s characteristics would impact your organization. Key questions include: Does the 10-year benchmark stability and expanded payment flexibility make LEAD more attractive than your current arrangement (e.g. MSSP or Next Gen)? Can your organization commit to performance through 2036? For ACOs that have benefited from historical shared savings, locking in a favorable benchmark for 10 years could be very advantageous. On the other hand, LEAD’s mandatory discount in the Global track and new requirements (like the larger financial guarantee) need careful financial analysis.
- Gauge Your Readiness: Identify gaps between LEAD’s participation requirements and your current capabilities. For instance, ensure you have or can obtain the required 2-4% financial guarantee backing. Strengthen your provider network alignment – remember, LEAD uses full-TIN participation, so now is the time to confirm that all providers under each TIN are on board and to restructure any arrangements if needed. If you intend to pursue advanced payment options or capitation, engage your finance and billing teams to plan the operational changes (e.g., managing capitated payment streams and reduced FFS claim payments). Make sure your data systems can handle the reporting demands and that you have a game plan for quality measure performance under the new scoring approach.
- Consider Partnerships (especially for specialty care): LEAD provides novel ways to work with specialists and community providers. Primary care-centric ACOs should start conversations with high-volume specialists about Preferred Provider or NPCC arrangements – for example, collaborating with a nephrology group or orthopedic surgeons under a sub-capitation or CARA episode contract. Conversely, specialty groups not in ACOs might use LEAD as an entry point (either by joining an ACO or leading one focused on their patient population). The next article in this series will explore strategies for specialist practices in detail, but ACOs can begin identifying key specialists who manage high-cost conditions among their patients and explore mutual opportunities in LEAD’s framework.
- Submit Your Application or LOI: If you are strongly interested and meet the criteria, don’t miss the May 17, 2026, deadline for applications. The application will require detailed information, including your organizational structure, governance, clinical model, and plans for using LEAD’s features (capitation choices, benefit enhancements, etc.). Assemble a dedicated team to work on it now and reach out to legal and financial advisors as needed, given the complexity of the RFA. For those not ready this year, submitting an LOI by April 20 is a good idea – it keeps you on CMS’s radar for future cohorts and may give you access to additional info sessions or technical assistance. But keep in mind that future application rounds may have different requirements or more limited slots. The safest way to guarantee a place in this model under the most favorable terms is to join in its inaugural year.
The LEAD Model is poised to be the flagship federal ACO program for the next decade, with CMS aiming to broaden participation and drive sustaining transformations in care delivery. It offers forward-thinking ACOs a rare combination of long-term predictability and new financial tools to manage patient care. With the RFA now in hand, ACO leaders should quickly determine if LEAD aligns with their strategic goals. For many, this will mean seizing the chance to apply now and shape the next chapter of value-based care.
This client alert is the first in a four-part series on the Innovation Center LEAD Model. Upcoming alerts will dive deeper into: (1) opportunities and considerations for specialist physician practices under LEAD; (2) a detailed comparison of ACO REACH vs. LEAD and what the transition means for different organizations; and (3) nephrology-specific perspectives on LEAD (implications for CKD/ESRD care and how LEAD differs from kidney models like CKCC and the new ACCESS initiative).
Key CMS Resources – LEAD Model
For clients who want to go directly to CMS sources, the most useful publicly available documents are:
LEAD Model Application & Supporting Documents (CMS)
- LEAD Model Request for Applications (RFA) (PDF)
- LEAD Application Submission Portal
- LEAD Model Application Checklist (PDF)
- LEAD Model Payment Factsheet (PDF)
- LEAD Model Overview Factsheet (PDF)
- LEAD Model Value Factsheet (PDF)
- LEAD Model Overview Webinar Slides (PDF)
- LEAD Model Overview Webinar Transcript
- CMS‑Administered Risk Arrangements (CARA) Factsheet (PDF)
The Benesch Healthcare practice team monitors developments related to the LEAD Model and other CMMI initiatives and may provide additional updates as they become available. Please contact the authors of this article for additional information or if you have any questions.
[1]Long‑term Enhanced Accountable Care Organization Design (LEAD) Model Request for Applications, CTRS. FOR MEDICARE & MEDICAID SERVS. (Mar. 31, 2026), https://www.cms.gov/priorities/innovation/files/lead-rfa.pdf.
[2]Payment Factsheet for the Long‑term Enhanced Accountable Care Organization Design (LEAD) Model, CTRS. FOR MEDICARE & MEDICAID SERVS., https://www.cms.gov/priorities/innovation/files/lead-payment-fs.pdf.
[3]CMS‑Administered Risk Arrangements (CARA) Factsheet, CTRS. FOR MEDICARE & MEDICAID SERVS.,
https://www.cms.gov/priorities/innovation/files/lead-cara-fs.pdf.
[4]Innovation Insight: CMS Invites ACOs to Apply to the New LEAD Model, CTRS. FOR MEDICARE & MEDICAID SERVS. (Mar. 31, 2026), https://www.cms.gov/priorities/innovation/innovation-insight-cms-invites-acos-apply-new-lead-model.